
Executive Summary
Under the Canadian constitution, provincial governments bear primary responsibility for the delivery of health care and often develop their own strategies to address mental health and addiction. In practice, however, local governments shoulder much of the burden of front-line service delivery, often with limited fiscal resources. With rising rates of mortality due to opioid addictions, and the substantial costs of mental illness – not just to the health care system but also to the social and economic well-being of Canadians – urgent coordinated action is needed.
The two essays in this paper set out the municipal role in harm reduction and mental well-being and provide recommendations for action. They argue that while municipalities have a lead role to play, cooperation with other local agencies and other orders of government is essential.
Municipalities
R. Marcus Hammond, Barb Fornssler, and Elaine Hyshka examine how municipalities can effectively respond to substance-related harm through a harm reduction approach. They argue that Canadian municipalities are well positioned to implement harm reduction policies, programs, and practices across key governance domains and through enhanced intergovernmental cooperation. They provide recommendations for organizational policies and procedures, zoning and land use planning, direct service delivery, and drug policy and enforcement reform that municipalities can adopt to reduce morbidity and mitigate impacts on people, families, and communities.
Kwame McKenzie, Rishika Wadehra, Sophie Baker, and Jesse Rosenberg note that municipalities have a front-line role in, and unique perspective on, many social factors that can impact mental health and well-being, including housing and homelessness, racism, climate change, substance use and addictions, and public safety. They recommend that municipalities, as the order of government that knows their context and populations best, bring leaders and communities together and leverage their networks, including community organizations and health-care providers, to develop effective approaches – and they offer a practical blueprint for doing so. McKenzie et al. also provide case studies of cities which have taken leadership roles in well-being.
Provincial governments
Hammond, Fornssler, and Hyshka note that policy support across provinces and territories is variable. Their recommendations include advocating for harm reduction policies and funding from provincial and federal governments; developing local substance strategies with provincial and community partners; and establishing communications and data-sharing mechanisms with all orders of government over the long term to ensure timely release of policies and health data.
McKenzie et al. suggest that all orders of government must widen their focus to consider both population and risk-reduction approaches, including not only making targeted interventions but acting on the structural and social determinants of health to foster greater well-being. Given that many policy and funding levers are provincial in jurisdiction, municipalities can advocate for policy and funding changes to drive progress. This paper also points to the role provinces can play in collecting and providing additional data and making it accessible.
Federal government
Hammond, Fornssler, and Hyshka note that a harm reduction approach to enforcement and drug policy reform should prioritize connecting people to services rather than punishing them. Accordingly, they recommend decriminalization for minor drug offences alongside other harm reduction approaches, while noting this policy has been controversial to date in areas where it has been tried.
McKenzie et al. recommend that the federal government provide funding directly to municipalities and civil society groups to lead efforts on well-being.
Intergovernmental Cooperation
In both essays in this report, the authors strongly recommend intergovernmental cooperation in a range of areas, including in policy areas that are not within (or solely within) municipal jurisdiction (e.g., criminal justice, income supports, schools, job training). Both essays also argue that enhanced intergovernmental cooperation in the areas of data sharing, funding, and service delivery is needed to more effectively reduce harm and improve mental well-being.
Backgrounder: Municipalities and Mental Health
By Gabriel Eidelman, Rong Zhang, and Nick Pearce
Gabriel Eidelman is Assistant Professor, Teaching Stream, and Director of the Urban Policy Lab at the Munk School of Global Affairs and Public Policy.
Rong Zhang is a recent graduate of the Master of Public Policy program at the Munk School of Global Affairs and Public Policy.
Nick Pearce is a recent graduate of the Master of Global Affairs program at the Munk School of Global Affairs and Public Policy.
Introduction
Mental health refers to an individual’s psychological and social well-being. People suffering from poor mental health are dealing with emotional challenges, such as stress, loneliness, stigma, discrimination, pain, or trauma, that in some cases can lead to more severe mental illnesses or medical conditions, including depression, eating disorders, post-traumatic stress disorder, and substance use disorders. More than 5 million Canadians experience significant symptoms of mental illness.[1] In recent years, more than 4,500 people in Canada have died annually by suicide, and more than 5,500 from opioid poisoning.[2]
Improving people’s mental health requires access to health care services (e.g., counselling, psychiatric treatment) and social services (e.g., income supports, services for people with disabilities); both categories of services fall primarily under provincial jurisdiction based on the Constitution Act, 1867.[3] The federal government helps fund these services and encourages policy coordination between provincial governments through a range of legislative frameworks, regulatory standards, and fiscal transfers. For example, the Canada Health Act states that the objective of health care policy is to “restore the physical and mental well-being” of Canadians (emphasis added), and sets out standards for provincial and territorial implementation of “medically necessary” mental health services.[4] Provinces deliver these services in accordance with their own mental health laws, each of which specifies protocols for psychiatric treatment in its jurisdiction (e.g., Ontario’s Mental Health Act), as well as province-specific mental health strategies (e.g., Manitoba’s Pathway to Wellness Strategy).[5]
Although not formally responsible for mental health, municipal governments in Canada are nevertheless at the front lines of what many experts describe as a mental health crisis
Although not formally responsible for mental health, municipal governments in Canada are nevertheless at the front lines of what many experts describe as a mental health crisis.[6] As the order of government “closest to the people,” municipalities must grapple with increasing rates of homelessness, poverty, and addiction, while also shouldering a growing share of the burden of delivering mental health services.[7]
Local governments provide a range of services that acutely impact people’s mental health, such as housing (see Who Does What report No. 1, April 2022), public health (Who Does What report No. 4, November 2022), and policing (Who Does What report No. 5, December 2022), as well as local services with indirect effects, such as parks and public spaces. Some also deliver specialized mental health services and support programs, including crisis response teams, suicide prevention units, counselling services, harm reduction and safe injection sites, addiction treatment centres, and supportive housing.
This backgrounder outlines the role municipalities play in delivering mental health services for Canadians. First, it examines mental health initiatives municipalities have taken on their own, as policy-makers, direct service providers, and employers. It then describes instances of municipalities collaborating with provincial and federal governments within Canada’s broader mental health system.
Independent municipal action within legal and fiscal constraints
A handful of municipalities across Canada have adopted dedicated mental health strategies and policy frameworks that prioritize the social determinants of health and treatment for substance use. In 2023, Toronto City Council adopted a mental health strategy for improving access to quality housing, exposure to green space, and nutritious food.[8] Calgary’s Mental Health and Addiction Strategy, adopted in 2021, includes a mental health survey and funding for research partnerships and community initiatives.[9] Many more municipalities, including Edmonton, Ottawa, Hamilton, and Regina, have adopted Community Safety and Well-Being Plans setting out the role of police services with respect to mental health and established crisis intervention protocols for people experiencing mental distress.[10]
Beyond setting policy, local governments deliver many mental health services directly. For example, Montréal’s municipal court, a tribunal that hears some civil, criminal, and administrative offences within city limits, operates the Programme d’accompagnement justice et santé mentale to monitor and support people who are struggling with mental health issues and substance use while facing charges.[11] The City of Hamilton’s services include street outreach services for those experiencing homelessness as well as case management from a team of public health nurses for those with serious mental health concerns and no fixed address.[12] Toronto recently introduced Canada’s first Community Crisis Service, including a 211 mental health crisis line (distinct from its 911 emergency service), which dispatches a mobile crisis intervention team made up of nurses and mental health support workers – not police officers – to conduct wellness checks and respond to people in mental distress.[13]
Many municipal initiatives involve partnerships with business, civil society, and community groups. For example, Calgary’s “Connect the Dot” program funds a range of mental health initiatives, including multicultural mental health interventions for newcomers, youth, Indigenous elders, and people with disabilities, in collaboration with more than two dozen community organizations.[14] Likewise, Québec City partnered with Sun Life Financial to fund local agencies with mental health missions to provide outreach to 7,000 local youths.[15]
A handful of municipalities across Canada have adopted dedicated mental health strategies and policy frameworks that prioritize the social determinants of health and treatment for substance use.
Finally, as major employers, municipalities are also responsible for ensuring mental well-being among their workers. The COVID-19 pandemic and growing rates of addiction and homelessness in cities have taken a toll on municipal public servants. The Mental Health Commission of Canada confirms that municipal governments are experiencing lower productivity and greater absenteeism stemming from poor employee wellness.[16] Many midsize and large municipalities, including Halifax, Kitchener, Winnipeg, and Saskatoon, therefore provide their workers with access to corporate employee assistance programs, which offer short-term counselling and referral services.
All of these municipal initiatives are limited by tight fiscal constraints. Former Toronto Mayor John Tory observed that mental health responsibilities have effectively been “off-loaded” to local governments without adequate funding, a criticism echoed by the City’s expert Mental Health Roundtable, which noted the insufficiency of city resources for shelter services and supportive housing, 24/7 mental health care, and substance use crisis centres.[17] Ontario’s Big City Mayors caucus has publicly complained that municipalities lack the fiscal resources and capacity to address chronic homelessness and addiction issues.[18] At the national level, the Federation of Canadian Municipalities has campaigned for a new municipal fiscal framework to respond to the mental health crisis.[19]
Municipal action is also constrained by legal and regulatory restrictions. For example, in 2022, the City of Vancouver requested an exemption to the federal Controlled Drugs and Substances Act to decriminalize simple possession of illicit drugs (people using or carrying small amounts of drugs for personal use), consistent with its efforts to treat drug addiction as a public health, rather than law enforcement, problem. The province and federal government granted the exemption in January 2023, but revoked it in May 2024 due to public pressure.[20] Similarly, Ontario recently announced the closure of 10 of the province’s 23 supervised drug consumption sites, including locations operated by the municipal public health units in Toronto and Kitchener.[21] The Safer Streets, Stronger Communities Act, 2024, prohibits municipalities from applying to the federal government to decriminalize illegal drugs.[22]
Municipal collaboration with other orders of government
As a result of both financial and legal constraints, municipal governments must work closely with provincial health authorities. [PR2] For example, Vancouver relies on its regional public health authority, Vancouver Coastal Health (VCH), to deliver treatment options and mental health services. VCH and the City of Vancouver serve as co-chairs of the Vancouver Community Action Team, a cross-sector advisory table with representation from more than 25 community organizations, professional bodies, service providers, and individuals with lived experience.[23] Likewise, the City of Edmonton worked with Alberta Health Services to produce the Edmonton Suicide Prevention Strategy, developed by a multisectoral advisory committee.[24]
Housing is an important social determinant of health, and municipalities also collaborate with provinces on supportive housing programs. In 2023, the Government of Saskatchewan allocated $40.2 million for 155 new supportive housing spaces and $14.1 million for 120 additional emergency shelter spaces and permanent emergency shelters in Saskatoon, Regina, Prince Albert, Moose Jaw, and other communities.[25] Municipal governments worked with the Province to identify appropriate locations to deliver these services and to mitigate community safety issues. Meanwhile in British Columbia, the provincial government worked with the City of Vancouver to create 350 new permanent supportive homes on municipally owned land. The City was responsible for providing sites and coordinating service providers, while a provincial agency, BC Housing, provided funding and managed construction.[26]
Occasionally, municipal governments convene intergovernmental forums for collaboration around mental health. In 2021, the Federation of Canadian Municipalities hosted a virtual roundtable, part of its IMFG-supported Urban Project, to connect big-city mayors with provincial and federal representatives to share lessons in mental health responses and explore the barriers to, and opportunities for, greater collective action and mobilization.[27] Ontario’s Big City Mayors (OBCM) caucus also routinely raises mental health priorities with provincial officials, and has developed an advocacy campaign (SolvetheCrisis.ca) to encourage action.[28] But this kind of intergovernmental engagement is typically ad hoc and difficult to sustain.
Conclusion
In summary, municipalities play an important and growing role in addressing the mental health crisis in Canada. Several local governments have developed and implemented dedicated mental health strategies, and many more either directly deliver mental health services that benefit residents or contribute to these services in other ways. However, these efforts are often hampered by funding, legislative, and regulatory challenges, raising the question of whether federal and provincial governments should empower local governments to do more, or relieve them of the political and financial burden of improving residents’ mental and social well-being.
Substance Use Governance in Canada: Considerations for Advancing Municipal Harm Reduction Policy and Intergovernmental Cooperation
By R. Marcus Hammond, Dr. Barb Fornssler, and Dr. Elaine Hyshka
R. Marcus Hammond is an applied health researcher and registered psychiatric nurse, and a Master of Science student at the School of Public Health, University of Alberta.
Dr. Barb Fornssler is an Assistant Professor and Director of the Substance Use Health and Wellbeing Certificate Program at the School of Public Health, University of Saskatchewan.
Dr. Elaine Hyshka is an Associate Professor and Canada Research Chair in Health Systems Innovation at the School of Public Health, University of Alberta.
Since 2016, more than 50,000 people have died of apparent opioid toxicity in Canada.[29] From January to September of 2024, Ontario, Alberta, and British Columbia have accounted for the majority (upwards of 83%) of opioid toxicity deaths nationally.[30]Complex antecedents contribute to drug poisoning deaths; however, the substantial rise in mortality observed since 2014 primarily reflects a fundamental shift in the illegal drug market toward novel synthetic opioids, including fentanyl, which have made drug use significantly more unpredictable and dangerous.[31] Harm reduction is a critical component of an effective response to the toxic-drug crisis.[32]
In this article, we provide a brief overview of harm reduction and of the ways various orders of government in Canada have responded to substance-related harm, with a central focus on municipal governance. We consider how municipalities are aptly positioned to effectively respond to, and address, substance-related harms in real time; what challenges may arise and how they can be navigated; how municipalities can better address – and anticipate – the needs of people who use substances (PWUS); and why intergovernmental cooperation is not only key to this endeavour but more crucial than ever before.
What is harm reduction and how does it relate to municipal governance?
Harm reduction is a philosophy of care and a set of strategies focused on promoting the health and safety of PWUS – including alcohol and inhalants, regulated drugs (e.g., cannabis, opioids, and hallucinogens), and unregulated drugs (e.g., fentanyl-like drugs, heroin, and methamphetamine) – as well as those with a history of substance use (i.e., people who are in recovery).[33] It is one component of a comprehensive public health approach to substance use and aims to minimize the negative health, social, and legal impacts associated with substance use, drug policies, and drug laws.[34] Harm reduction comprises policies, programs, and practices that focus on positive change and on connecting to people without judgment, coercion, or discrimination – and without requiring that they stop using drugs as a precondition of support.[35] Robust evidence demonstrates that harm reduction services (such as needle and syringe distribution, supervised consumption sites, and naloxone programs) reduce substance-related morbidity and mortality, as well as the risk of infectious diseases such as HIV and Hepatitis C.[36]
Provinces and territories are primarily responsible for the administration, funding, and delivery of health services in Canada. However, health care is a shared jurisdiction; federal legislation (e.g., the Canada Health Act), policy, and spending programs are important influences on provincial and territorial decision-making.
Although the federal Canadian Drugs and Substances Strategy[37]endorses harm reduction as an important component for effectively responding to substance-related harms, policy support across provinces and territories is more variable. And despite being the nearest order of government to the daily lives of local citizens, municipalities often do not have any formal harm reduction policies.[38] In response, while mechanisms for strengthening intergovernmental cooperation are essential, municipalities that innovate, adapt, and implement locally relevant harm reduction responses to the toxic drug crisis and other substance-related harms have the potential to reduce substance-related morbidity and mortality and to mitigate impacts on people, families, and communities.
In summary:
- Harm reduction focuses on positive change and minimizing negative impacts of substance use.
- Evidence-based interventions include education about safer substance use, access to sterile substance use supplies including life-saving naloxone, and access to supervised consumption services.
- All orders of government are equipped to respond to substance-related harm, including through administration, funding, and health and social-service delivery.
- Municipalities are well positioned to adapt and implement locally appropriate harm reduction responses to substance-related harms.
A targeted approach for advancing harm reduction locally: Four key municipal policy levers
Organizational policies and procedures
Organizational policies and procedures are the formal guidelines, rules, and practices established by an entity (municipality, business, etc.) to govern its internal operations and ensure consistency and efficiency in delivering services. Where possible, municipalities should consider applying a harm reduction lens to relevant policies and procedures to ensure that they promote the health and well-being of PWUS. [PR4]
For example, in 2020 the City of Toronto passed a naloxone administrationpolicy enabling designated city employees to administer naloxone in the event of an emergency.[39] As of June 1, 2023, Ontario was the first jurisdiction in North America to mandate at-risk workplaces to carry naloxone. Working in tandem with the provincial directives, many business owners and city employees in Thunder Bay – a region disproportionately impacted by drug toxicity deaths in recent years – have received naloxone training through Ontario’s Workplace Naloxone Program so as to be prepared in the event of an emergency.[40] Ongoing monitoring, evaluation, and intergovernmental cooperation strategies can help assess the effectiveness of this program in Thunder Bay and offer recommendations for refinement. Unfortunately, other municipalities have taken steps to formally prohibit employees from carrying naloxone at work. The City of Edmonton announced a policy prohibiting most city employees from administering naloxone during work hours due to fears regarding potential legal liability.[41] These concerns stand in contrast, however, to widespread employer support for the deployment of automated external defibrillators and cardiopulmonary resuscitation in the event of a medical emergency. Furthermore, evidence shows that bystanders can safely recognize an overdose and administer naloxone as part of emergency first aid.[42] And while naloxone is typically administered via an intramuscular injection, it is also available in an intranasal formulation for workplaces seeking to further reduce the risk of unintended adverse events, such as needle stick injuries.[43]
The way forward includes raising awareness of harm reduction measures through community engagement and partnerships with non-governmental organizations, health agencies, and other community groups in order to address stigma and garner resources, expertise, and public support for organizational policy development.
Bylaws and land use planning
Bylaws are enforceable laws enacted by local authorities to regulate activities within a given jurisdiction; land use planning is the process by which municipalities regulate land use and development within their jurisdictional boundaries through zoning bylaws that designate specific areas for certain uses or purposes.[44] A harm reduction approach to municipal zoning and land use planning wouldensure that services for PWUS are treated in accordance with regulations applied to other health and social services while further identifying opportunities and key strategies for promoting their availability. For example, in Edmonton a health and wellness plan that includes harm reduction measures is required as part of the permit application process for electronic dance music parties and other events where substance use is likely to occur.[45]
As key catalyzers of concerted policy adoption, municipalities are well positioned to lead the change through inclusive and non-stigmatizing approaches to substance use, including the consistent application of regulations applied to other health and social services.
While bylaws and land use planning tend to govern space according to use or activity, they also tend to organize and govern certain groups (for example, people experiencing unsheltered homelessness) via the regulation of public spaces.[46] Recently in Edmonton, amendments were passed to the Public Spaces Bylaw 20700 to ban loitering on transit, panhandling by roadways, and to impose fines of up to $25 for openly possessing or consuming a controlled substance anywhere in public. However other infractions related to houselessness may incur fines of up to $250.[47] However, such bylaws are not only discriminatory but largely ineffective. They tend to target certain groups of PWUS without addressing core issues (e.g., housing insecurity, a lack of safe consumption sites); they create redundant sanctions on something already criminalized; they further entrench people in poverty with fines they cannot pay; and they increase the risk of harm for PWUS experiencing homelessness, who may respond to increased enforcement by using drugs in more concealed and isolated areas, reducing the chances of a timely response to an overdose. Despite the development of such prohibitive public spaces, the City of Edmonton recently made permanent a pilot program allowing permit holders to legally consume alcohol at picnic sites in some parks around the city.[48] While this program may be beneficial as it represents a small step in the direction of reducing substance use stigma, this differentially targeting of certain groups of PWUS over others prioritizes a punitive rather than public health approach to substance use, leading to further stigma, inequities, and harm. Elsewhere in Canada, some municipalities have sought to pass bylaws that ban development permits for harm reduction or substance use treatment services.[49]
These examples highlight how municipal land use planning can reinforce stigma against people who use drugs.[50] As key catalyzers of concerted policy adoption, municipalities are well positioned to lead the change through inclusive and non-stigmatizing approaches to substance use, including the consistent application of regulations applied to other health and social services.
Funding and service delivery
Many municipalities fund community-service programs supporting the health and well-being of their citizens. Although provincial and territorial tax revenue is typically the main source of funding health services, municipalities can also directly fund and/or deliver harm reduction services such as overdose prevention sites and supervised consumption services, needle distribution programs, and outreach programs.[51] They may, however, hesitate to adopt this approach due to political and public resistance, ongoing funding constraints, competing municipal priorities, and the challenges of coordinating effective and continuous care between departments and organizations.
In one example of rising to this challenge, the City of Regina recently announced an innovative harm reduction funding strategy that enables community stakeholders to pilot projects, hire staff, and adapt services to fill in the gaps within provincially funded services.[52] Ontario’s municipalities are in a unique situation in that they are responsible for delivering local public health services directly, with funding and support from the provincial government.[53] This arrangement enables further municipal innovation in the substance use and harm reduction space. For example, despite challenges securing resources, funding, and community support, the City of Peterborough began actively working toward implementing a consumption and treatment service site as early as 2018; the site officially opened June 13, 2022.[54]Within the first year of operations, it prevented more than 70 drug-related fatalities, had over 10,000 unique visits, and connected with over 300 unique clients.[55]
Enforcement and drug policy
A final municipal policy lever involves federal drug laws and their enforcement through local policing, law enforcement, and criminal justice.[56] Criminalizing drug use has been shown to exacerbate harm by discouraging help-seeking, making it harder to search for housing and employment while also driving public drug use into increasingly secluded spaces.[57] In contrast, a harm reduction approach to enforcement and drug policy considers the health and safety of all PWUS by prioritizing connecting people to services rather than punishing them.[58]
Decriminalization as an approach to reforming enforcement and drug policy can include a range of principles, policies, and practices that remove the application of criminal and/or administrative penalties for minor drug offenses (see Figure 1).[59] Decriminalization alone may not be sufficient to improve a population’s health; however, alongside harm reduction approaches, a decriminalization policy approach has been shown to reduce new HIV infection diagnoses linked to drug injection, and to mitigate overdose mortality and other drug-related harms associated with criminal justice prosecution for simple possession.[60]
Figure 1: The regulatory continuum
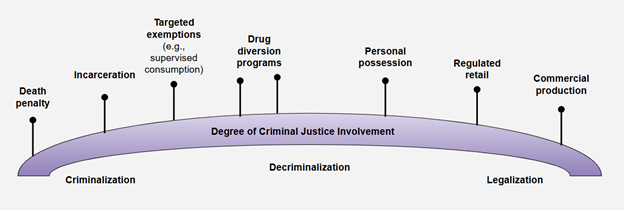
Source: Adapted from Rebecca Jesseman and Doris Payer, Decriminalization: Options and Evidence (Ottawa: Canadian Centre on Substance Use and Addiction, 2018).
In line with this approach, in 2020 the Canadian Association of Chiefs of Police endorsed alternatives to criminal sanctions for simple possession, and multiple municipalities in Canada have recently taken steps toward decriminalizing minor drug possession through section-56 exemptions to the Controlled Drugs and Substance Act.[61] However, federal policy to date has not been consistently supportive of this approach, and provincial governments have thrown up roadblocks that hinder municipalities pursuing it. The challenges to garnering consistent intergovernmental support are highlighted by the experience of the City of Edmonton, whose councillors voted in 2022 to develop a decriminalization strategy for simple personal possession. The Government of Alberta – along with the Alberta Association of Chiefs of Police – responded with significant opposition, calling the move premature and citing community safety concerns.[62] And while British Columbia enacted a decriminalization pilot policy in 2023, it retracted elements of it within a year following public backlash.[63]
A potential alternative model for municipalities facing resistance to decriminalization is the Law Enforcement Assisted Diversion (LEAD) program, which has been implemented across the United States. LEAD is a police-led response where, in lieu of laying drug possession charges, police officers connect PWUS with community supports such as housing, medical care, mental health supports, job training, and additional services.[64]
Conclusion: A broad approach for advancing harm reduction policy through intergovernmental cooperation
While conventional thinking has been that health services often fall outside the purview of municipal governance, the severity of Canada’s drug toxicity crisis – and other substance-related harms – challenges all orders of government to work together toward a comprehensive approach.
Our recommendations for both urgent action and long-term implementation are summarized in Table 1. Although they are oriented for municipalities, all orders of government are encouraged to do their part while working cooperatively to make these actions reality.
Table 1: Recommendations for action
| Short-Term (Urgent) | Long-Term | |
|---|---|---|
| Advocate for harm reduction policies at the municipal, provincial, and federal levels to better ensure that resources are available for local communities.[65] | Establish key communication pathways and data-sharing mechanisms across federal, provincial, and municipal governments. | |
| Develop local substance strategies in collaboration with provincial and community partners.[66] | Ensure that adopted policies and strategies, including relevant health data, are released in a timely manner. | |
| Enact relevant policies and procedures that enable employees to carry and use naloxone in the workplace. | Create coalitions and partnerships with other municipalities across Canada. | |
| Ensure local police services are engaged with drug policy reform, equipped to deal with overdoses – in terms of both equipment and staff training – and supported in building cooperative partnerships with harm reduction services.[67] | Implement programs that provide job training and employment opportunities for PWUS and those living in recovery. | |
| Extend the reach of municipal services for PWUS | Provide employees with access to evidence-based substance-use care through employer-provided benefit programs (e.g., harm reduction education and resources, such as take-home naloxone programs; medication treatments, such as buprenorphine and naltrexone; and other effective counselling and psychosocial supports). | |
| Apply for integrated measures related to drug policy reform (e.g., decriminalization of simple possession; development of LEAD or similar police-based diversion initiatives; implementation of supervised consumption facilities; and expansion of services and supports that bridge the mutual goals of ensuring the public is healthy and safe). | ||
| Develop and implement robust program evaluation strategies to track performance across multiple measures, and refine them as needed going forward. | ||
By integrating both a targeted short-term focus and a broad long-term approach to municipal substance use and harm reduction governance in Canada, we emphasize how a comprehensive, intergovernmental way forward can not only mitigate the drug toxicity crisis and other substance-related harms where the impacts are most egregious – among people, families, and their communities – but also foster personal resilience and healing along with community renewal.
The Case for Municipal Action on Mental Well-Being
By Kwame McKenzie, Rishika Wadehra, Sophie Baker, and Jesse Rosenberg
Dr. Kwame McKenzie is CEO of Wellesley Institute, a full Professor in the Department of Psychiatry at the University of Toronto, Director of Health Equity at the Centre for Addiction and Mental Health (CAMH), and a practising psychiatrist.
Rishika Wadehra holds a Master of Public Policy from the Munk School of Global Affairs and Public Policy at the University of Toronto.
Dr. Sophie Baker is a researcher at Wellesley Institute working on the Thrive Toronto project with research interests in addressing mental health inequities.
Jesse Rosenberg is the Director of Policy at Wellesley Institute and a legal and policy professional with political and policy experience in the fields of health, labour, and justice.
Introduction
Mental health is not just the absence of mental illness. It encompasses an individual’s emotional, psychological, and social well-being, and it influences how they act, think, and feel.[68] The World Health Organization (WHO) defines mental health as “a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community.”[69] It is useful to think about mental health as existing on a scale from optimal mental health (flourishing) to poor mental health (languishing). The “two continua model” of mental health recognizes that individuals with and without a mental illness can flourish or languish.[70]
The health, social, and economic costs of poor mental health are substantial. Mental and physical well-being are closely linked: individuals with mental illness are at a higher risk of developing physical health conditions, and conversely, those with physical health conditions have an increased risk of mental illness.[71] Individuals with mental illness are at excess risk of substance use issues, and mental ill health has also been estimated to reduce life expectancy by 10 to 20 years.[72] Poor mental well-being has a negative effect on the social fabric of communities. The relationship between mental health and social capital is cyclical: poor mental health erodes social capital, and the deterioration of social capital, in turn, detrimentally impacts the overall well-being of communities.[73] In terms of economic consequences, in Canada, mental illness has been estimated to cost at least $50 billion per year; this includes the associated health-care costs, declining health-related quality of life, and productivity loss.[74]
The relationship between mental health and social capital is cyclical: poor mental health erodes social capital, and the deterioration of social capital, in turn, detrimentally impacts the overall well-being of communities.
The risk of poor mental health is not equally distributed across the population. Structurally disadvantaged communities, including Indigenous peoples, Black and other racialized communities, 2SLGBTQ+ people, people with a disability, and newcomer and refugee populations, experience poorer mental health outcomes.[75] The excess mental ill health in these populations is precipitated and maintained by inequitable access to the social determinants associated with living a healthy life, including nutritious food, economic security, quality housing, transportation, health care, personal care, and opportunities for social participation.
Barriers to accessing these social determinants represent a clear risk factor for experiencing adverse childhood experiences (ACEs), defined as traumatic and stressful events occurring in childhood and youth (ages 1 to 17).[76] Experiences of ACEs include abuse (physical, emotional, or sexual), neglect, and community violence. ACEs also encompass household dysfunction, which might include exposure to mental illness, substance abuse, or intimate partner violence. Extensive evidence demonstrates that ACEs are a strong predictor of later mental health and substance use issues.[77] Calculations of population attributable risks have estimated that removal of exposure to ACEs would prevent 28 percent of cases of psychiatric disorders in children and adolescents and 30 percent in adults.[78]
To develop effective approaches to improving mental wellness, all orders of government and the broader sector must widen their focus to consider both population and risk-reduction approaches. Depicted in Figure 2, Rose’s prevention theory suggests that improving the health of the whole population benefits more people than an approach based exclusively on risk reduction in which the high-risk population is shifted to within a lower-risk range.[79] This whole-population approach incorporates targeted interventions to support those at heightened risk of, or already experiencing, mental health issues, but also looks upstream and acts on the structural and social determinants of health to create conditions that foster greater mental well-being for all. This includes taking action to reduce the risk of exposure to ACEs. While action on mental well-being requires a multi-sectoral, public health approach that includes the whole of government in addition to civil society groups, businesses, and individuals, municipalities can and should play a leading role.
Figure 2: Rose’s prevention theory
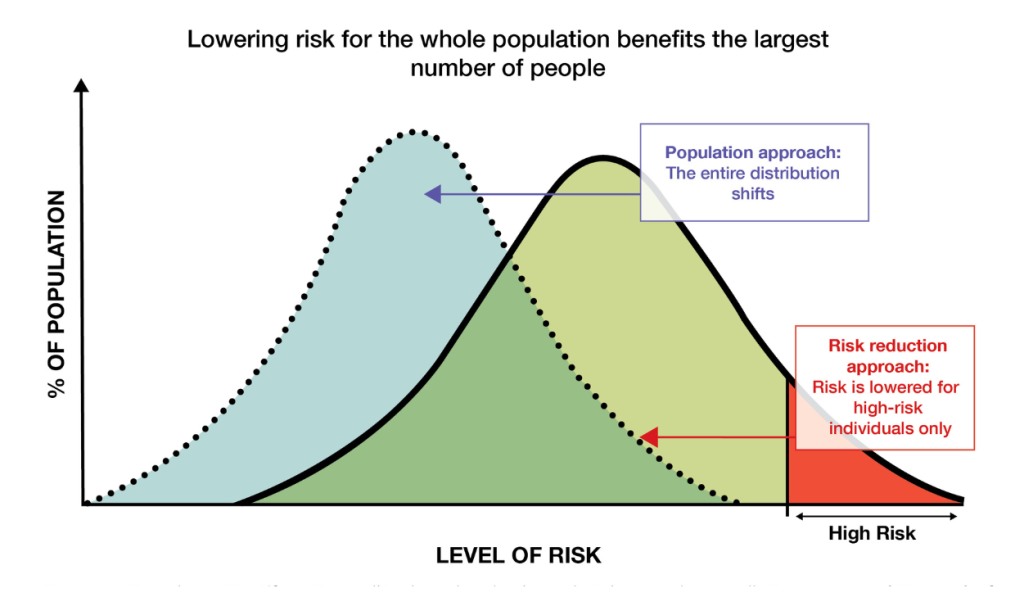
Source: Geoffrey Rose, “Sick individuals and sick populations,” International Journal of Epidemiology 14,1 (1985): 32–38. Retrieved from https://doi.org/10.1093/ije/14.1.32
Why should municipalities act on mental health and well-being?
Municipalities are the order of government often considered to be closest to their populations. They have a front-line role in, and a key perspective on, many social factors that can impact mental health and well-being, such as housing and homelessness, racism, climate change, substance use and addictions, and public safety.[80]
They often play a central role in social-service provision and in implementing the policies that can improve access to the critical social determinants of health. Although different municipalities have differing levels of involvement and varying capacities to provide social supports and services, given the range of responsibilities that provinces across the country have assigned to them, there are many opportunities for municipal leadership on mental health and well-being.
In addition to the opportunities in direct municipal work, municipalities can and should also take advantage of the many ways to lead through partnerships and engagement. There is evidence supporting the effectiveness of community interventions – defined as those involving multisector partnerships, community involvement, or service delivery in the community. These interventions focus both on individual mental health and on the determinants of mental health, aiming to improve mental health and social equity.[81] A review by Kirkbride and colleagues has also identified social determinants of mental health and primary prevention strategies across the life course that can be used to tackle mental health inequities.[82] Municipalities can leverage their networks, including community organizations and health-care providers, to develop effective approaches. Investment in mental health has also been found to have financial benefits – for example, by scaling up mental health programs and funding early-intervention programs targeting children and families.[83]
Recent data indicates a concerning decline in mental health across Canada. In addition to the pandemic, negative impacts on mental health have been driven by worsening inequality, a rising cost of living, and other social challenges that have been increasing in many cities across Canada, including Toronto, where at least 50 percent of people do not have sufficient income to live a healthy life.[84]
Yet governments in Canada have not made mental health a priority. While mental health funding varies across provinces and municipalities, federal spending in Canada lags behind that of other OECD countries.[85]
What examples exist?
Many municipalities, in Canada and beyond, have taken on leadership roles in well-being. The following four examples may be valuable inspirations.
Toronto, Ontario
The Our Health, Our City strategy was launched by the City of Toronto in 2023 with the aim of reducing substance-use-related harms and promoting mental health and well-being in the municipality; it includes recommended actions on improving mental well-being.[86] The THRIVE Toronto partnership was launched in 2017, and includes municipal partners and local leaders from multiple sectors that play a role in improving mental well-being and psychological health in the city.[87] In October 2023 it released Thrive Toronto: A Mental Health Plan for Our City, which outlined five key actions: creating a community mental health report card, developing a climate change and mental health strategy, making progress on supportive housing, enhancing employee mental health benefits and workplaces, and a establishing a virtual learning centre with tools and training.[88]
Calgary, Alberta
The City of Calgary convened with community members, organizations, and other stakeholders to develop a community-based strategy, based on the THRIVE model, that focused on promoting mental wellness and connecting more people to mental health resources.[89] The strategy was initially launched in 2019 and was later approved for funding by Calgary City Council in 2021. While Calgary’s strategy, like the previous examples, emphasizes community involvement and data collection, it also adds a focus on accountability and evaluation. The plan outlines an action to create an evaluation and reporting team consisting of evaluation specialists to help develop a framework to assess the strategy’s progress.
International Examples
Canadian cities are learning from international initiatives including Thrive NYC and Thrive LDN. Thrive NYC was launched in 2015 and convened a City Mental Health Council made up of over 20 city agencies from various government sectors, supported by a Community Services Board whose members represent a wide range of interests and lived experience.[90] Thrive LDN was launched in 2017 with a goal to ensure that all London residents have an equal opportunity to good mental health and well-being by bringing together partners from different sectors to prioritize a collective and sustainable approach toward improving public mental health.[91]
How can my municipality contribute?
Canadian municipalities have different capacities and operate in different provincial contexts. However, there are ways for every municipality to contribute.
The first step is for the municipality to examine its own work through a mental health and well-being lens. This process should include examining all city functions in the context of the social determinants of health and well-being. Municipalities should act to improve in areas where they fall short, both on their own and in concert with other partners in areas such as poverty reduction, promoting affordable and supportive housing, and anti-racism. This includes ensuring that municipal-led services are integrated with other government services – for example, by supporting civil society groups. Many municipalities are large and influential employers. Establishing the best possible workplace psychological health and safety practices for City staff, as well as for subcontracted or funded service providers, can make a significant difference to overall well-being not only for those workers, but for their families and communities, as well as for the municipal residents they work with and for every day.
Municipalities should also take steps to ensure that their services are trauma informed, so they can best serve and protect their intended targets. Wellesley Institute research has identified seven key steps in examining municipalities that have made progress on becoming trauma informed[92]:
- Partner with the community to launch a movement around becoming trauma informed.
- Establish a cross-sectoral collaborative task force.
- Engage, listen, and define priority issues and solutions.
- Build trauma-informed awareness, understanding, skill, and capacity.
- Transform structures, policies, protocols, programs, and practices.
- Measure, monitor, and evaluate from the start.
- Spread, scale up, and resource progress.
These important efforts toward becoming trauma-informed could be identified as a key part of the broader well-being commitments envisioned here, or they could proceed as integrated, but separate, efforts.
The second key step municipalities can take is to lead the way in bringing leaders and community together to find actions that can improve well-being. In previous work with the Federation of Canadian Municipalities (FCM), Wellesley Institute developed a guide to how Canadian municipalities can make a difference on well-being for their people by connecting various partners and stakeholders to develop coordinated actions that prioritize community-based initiatives and act on the social determinants of health.[93]
Wellesley and FCM developed a seven-step cycle for municipal leadership:
- Complete an environmental scan – Document services, systems, funding streams, programs, and policies relating to mental well-being across all orders of government to identify gaps and opportunities.
- Engage with community members and assess needs – Include a variety of stakeholders in discussions and decision-making processes, including people with lived experience of mental illness, health-care providers, social-development organizations, police, members of the local business, community and private sectors, and cultural organizations.
- Find partners and begin planning – Set clear goals and subgoals, and identify populations working in collaboration with the community partners identified in step 2.
- Establish leadership and accountability – Incorporate a leadership team that is responsible for directing and implementing the mental health initiative. Ideally, include community members.
- Define and choose impact indicators – Identify population-level health and social indicators that can be used to track the progress of programs, including measuring impact at the program level and collecting qualitative data.
- Conduct programs and activities – Align programs and activities with overall goals, subgoals, and priority areas. Use input from stakeholders to ensure that programs are equitable, community focused, and tailored to the diverse and evolving needs of different groups and regions.
- Evaluate outcomes – Implement ongoing evaluation to continue and evolve the strategy. This might include tracking population level data or using external organizations or an advisory group to oversee progress. After evaluation, these seven steps should be followed again.
Municipalities know their own contexts and populations best – they can and should adapt this advice to meet their own communities’ needs and capabilities.
Third and finally, municipalities can take action with respect to ACEs. Social inequities increase the likelihood of ACEs, which are significant risk factors for mental illness. Therefore, preventing and mitigating their impacts through upstream interventions should be an important part of addressing mental health inequities. Municipalities have an opportunity to do the difficult work of determining how their efforts can help.
How can other governments help?
Although there is much more all municipalities can do to improve their residents’ well-being, they should not have to do this work alone, given that many policy and funding levers are under the jurisdiction of provincial governments in Canada. Before, during, and after taking actions to help their populations thrive, municipalities can also advocate for policy and funding changes in other orders of government, with the commitments the municipality has taken on alone providing context.
Other orders of government should come to the table with municipalities. Schools, mental and physical health care, income supports, policing, access to green space outside the municipality, labour laws, minimum wages – there are a plethora of relevant areas that are outside, or at least not exclusive to, municipal jurisdiction. With the right provincial and federal leaders involved and committed to local well-being efforts, progress can be made much more quickly.
Other orders of government can also contribute by providing data. Specifically, they can 1) provide additional data that is available to provincial or federal governments, 2) make that data more easily accessible, and 3) collect new data that municipalities identify they need – ways to help to provide essential information for well-being efforts.
Finally, we also recommend that Canada’s federal and provincial governments provide funding directly to municipalities and civil society groups to lead efforts on well-being as discussed above.
Conclusion
Ensuring the mental health and well-being of their people is essential for all orders of government across Canada, and municipalities are well positioned to take action in this area. By assuming leadership roles, municipalities can generate significant dividends, including savings on municipal services, stronger economies with higher participation and productivity, and, most importantly, happier, healthier communities where individuals can thrive in the places they love to live.
About the Contributors

R. Marcus Hammond is an applied health researcher, a registered psychiatric nurse, and a Master of Science student in the Health Policy and Research stream at the University of Alberta’s School of Public Health. His interdisciplinary work spans applied research, practice, and policy to advance a public health approach to rural and urban health, substance use, and harm reduction. With experience advising municipal leaders in Canada and South Africa, he contributes to the development and scaling of systems innovations that improve health outcomes and promote equity. Marcus works closely with people with lived and living experience, service providers, health authorities, and local governments to support evidence-informed decision-making and inclusive policy development.

Dr. Barb Fornssler, PhD, is a white settler living on Treaty 6 territory and the homeland of the Métis, who works as an Assistant Faculty member in the School of Public Health at the University of Saskatchewan. Barb directs the Graduate Certificate in Substance Use Health and Wellbeing along with the Municipal Leadership in Addressing Substance Use Harms micro-credential at the University of Saskatchewan. She is the Knowledge Translation and Exchange coordinator for the CRISM Prairie Node. When she’s not in the community or the classroom, Barb enjoys camping adventures alongside her partner and their dogs, a Great Dane named Opal and a Lab named Kal. The family cat, Raziel, prefers to sunbathe at home in the living-room window.

Dr. Elaine Hyshka is an Associate Professor and Canada Research Chair in Health Systems Innovation at the University of Alberta’s School of Public Health, and Scientific Director of the Inner City Health and Wellness Program. Her program of health systems and services research is focused on advancing a public health approach to substance use in Canada. She works closely with service providers, health authorities, people with lived experience of substance use, and all orders of government to identify, evaluate, and scale systems innovations for improving health outcomes and advancing health equity.

Dr. Kwame McKenzie is CEO of Wellesley Institute, which works in research and policy to improve health and health equity in the Greater Toronto Area. A practising psychiatrist, he also holds positions as a full Professor at the University of Toronto and as Director of Health Equity at the Centre for Addiction and Mental Health (CAMH). As an international expert on the social causes of illness and the development of effective, equitable social policy and health services and systems, Dr. McKenzie has advised health, housing, education and social services ministers in Canada and the U.K. and has authored more than 280 peer-reviewed papers and six books. He is a member of Canada’s National Advisory Council on Poverty, Co-Chair of Ontario’s Black Health Plan, and Chair of the Board of Community Food Centres Canada. He has also worked as a consultant to the World Health Organization and the World Bank. Dr. McKenzie has been a columnist for The Guardian and The Times, a presenter for BBC Radio, and he is regularly published in the Toronto Star.

Rishika Wadehra holds a Master of Public Policy from the Munk School of Global Affairs and Public Policy at the University of Toronto. Her policy interests lie in the areas of health and social policy, including child care, education, immigration, and inequality. Through her work, she hopes to explore how public policy can confront growing inequities by considering the role of social determinants of health on the differential experiences of vulnerable populations.

Dr. Sophie Baker is a researcher at Wellesley Institute working on the Thrive Toronto project. Her research interests lie in addressing mental health inequities. Sophie completed her PhD in Psychology at Bangor University in the United Kingdom. Her research employed mixed methods to explore the interplay between minority group identity and mental health, with a specific focus on linguistic minority status. Sophie is also a member of the U.K. National Health Service’s Race and Health Observatory’s Mental Health Working Group, which is responsible for directing research and informing policy development to reduce mental health inequities in the United Kingdom.

Jesse Rosenberg is a legal and policy professional with political and policy experience in the fields of health, labour, and justice. Director of Policy at Wellesley Institute, Jesse previously held leadership roles with the government of Ontario and the Ontario College of Trades. He has extensive experience and expertise in stakeholder relations as well as legislative and regulatory development and analysis. He holds a Bachelor of Humanities from Carleton University and a Juris Doctor from Osgoode Hall.
Acknowledgements
R. Marcus Hammond, Barb Fornssler, and Elaine Hyshka would like to acknowledge all those impacted by the toxic drug poisoning crisis and municipal officials across Canada who are advocating for and prioritizing evidence-based responses in their jurisdictions.
About the Who Does What Series
Canadian municipalities play increasingly important roles in addressing policy challenges such as tackling climate change, increasing housing affordability, reforming policing, and confronting public health crises. The growing prominence of municipalities, however, has led to tensions over overlapping responsibilities with provincial and federal governments. Such “entanglement” between orders of government can result in poor coordination and opaque accountability. At the same time, combining the strengths and capabilities of different orders of government – whether in setting policy or in convening, funding, or delivering services – can lead to more effective action.
The Who Does What series gathers academics and practitioners to examine the role municipalities should play in key policy areas, the reforms required to ensure municipalities can deliver on their responsibilities, and the collaboration required among governments to meet the country’s challenges. It is produced by the Institute on Municipal Finance and Governance and the Urban Policy Lab.
About IMFG
The Institute on Municipal Finance and Governance (IMFG) is an academic research hub and non-partisan think tank based in the School of Cities at the University of Toronto.
IMFG focuses on the fiscal health and governance challenges facing large cities and city-regions. Its objective is to spark and inform public debate, and to engage the academic and policy communities around important issues of municipal finance and governance. The Institute conducts original research on issues facing cities in Canada and around the world; promotes high-level discussion among Canada’s government, academic, corporate, and community leaders through conferences and roundtables; and supports graduate and post-graduate students to build Canada’s cadre of municipal finance and governance experts. It is the only institute in Canada that focuses solely on municipal finance issues in large cities and city-regions.
IMFG is funded by the City of Toronto, the Regional Municipality of York, the Regional Municipality of Halton, the Regional Municipality of Durham, the Regional Municipality of Peel, Avana Capital Corporation, and Maytree.
About the Urban Policy Lab
The Urban Policy Lab is the Munk School of Global Affairs and Public Policy’s training ground for urban policy professionals, offering students career development and experiential learning opportunities through graduate fellowships, skills workshops, networking and mentorship programs, and collaborative research and civic education projects.
Endnotes
[1] Statistics Canada, “Mental disorders and access to mental health care, 2023.” Retrieved from https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00011-eng.htm
[2] Government of Canada, “Suicide in Canada,” 2024. Retrieved from https://www.canada.ca/en/public-health/services/suicide-prevention/suicide-canada.html; Government of Canada, “Opioid- and stimulant-related harms in Canada,” 2025. Retrieved from https://health-infobase.canada.ca/substance-related-harms/opioids-stimulants/
[3] Government of Canada, The Constitution Acts, 1867 to 1982, Justice Laws website, 2020. Retrieved from https://laws-lois.justice.gc.ca/eng/const/page-3.html#h-19; Canadian Public Health Association, A Public Health Approach to Population Mental Wellness, 2021. Retrieved from https://www.cpha.ca/public-health-approach-population-mental-wellness
[4] The Canada Health Act only applies to physician care and mental health services provided in hospital. This excludes counsellors, psychotherapists, peer support workers, and social workers working in the community. See Health Canada, Canada Health Act, 2023. Retrieved from https://www.canada.ca/en/health-canada/services/health-care-system/canada-health-care-system-medicare/canada-health-act.html.
[5] Government of Manitoba, A Pathway to Mental Health and Community Wellness: A Roadmap for Manitoba, 2022. Retrieved from https://www.gov.mb.ca/asset_library/en/mhcw/docs/roadmap.pdf
[6] Centre for Addiction and Mental Health, “The crisis is real,” 2025. Retrieved from https://www.camh.ca/en/driving-change/the-crisis-is-real
[7] Federation of Canadian Municipalities and Wellesley Institute, FCM Roadmap for Municipal Mental Health Initiatives, The Urban Project initiative, 2023. Retrieved from https://media.fcm.ca/documents/resources/Municipal-Mental-Health-Roadmap.pdf?_gl=1*6v1awj*_ga*MjA2NjYzNDg2NC4xNzA4MDI3OTA5*_ga_B4BFFLM1JF*MTcwODA5NDcyNi4yLjAuMTcwODA5NDgwNC42MC4wLjA
[8] City of Toronto, Our Health, Our City: A Mental Health, Substance Use, Harm Reduction and Treatment Strategy for Toronto, 2023. Retrieved from https://www.toronto.ca/wp-content/uploads/2023/11/977e-PublicHealthOurHealthOurCityMHAStrategy.pdf.
[9] City of Calgary, A Community of Connections: Calgary Mental Health and Addiction Community Strategy and Action Plan, 2021. Retrieved from https://www.calgary.ca/social-services/mental-health.html
[10] City of Edmonton, Community Safety and Well-Being Strategy, 2022. Retrieved from https://pub-edmonton.escribemeetings.com/filestream.ashx?DocumentId=146064; City of Ottawa, Emergency and Protective Services Department, Ottawa’s Community Safety and Well-Being Plan 2021–2031, 2021. Retrieved from https://documents.ottawa.ca/sites/default/files/CSWB_Plan_EN_.pdf; City of Hamilton, Hamilton’s Community Safety and Well-Being Plan, 2023. Retrieved from https://www.hamilton.ca/city-council/plans-strategies/strategies/community-safety-and-well-being-plan; City of Regina and Canadian Municipal Network on Crime Prevention, Community Safety and Well-Being Plan: Creating a Better Community Together, 2021. Retrieved from https://www.regina.ca/export/sites/Regina.ca/about-regina/community-safety-well-being/.galleries/pdfs/Community-Safety-and-Well-being-Plan.pdf;
[11] Ville de Montréal, “Municipal court: Social programs for the most vulnerable Montrealers,” May 25, 2023. Retrieved from https://montreal.ca/en/articles/municipal-court-social-programs-most-vulnerable-montrealers-49571
[12] City of Hamilton, “Mental health and street outreach program,” July 25, 2022. Retrieved from https://www.hamilton.ca/people-programs/public-health/mental-health-services/mental-health-street-outreach-program
[13] City of Toronto, “Toronto community crisis service,” 2025. Retrieved from https://www.toronto.ca/community-people/public-safety-alerts/community-safety-programs/toronto-community-crisis-service/
[14] City of Calgary, “Calgary’s mental health and addiction funding allocations,” n.d. Retrieved from https://www.calgary.ca/social-services/funding/prevention/funding-allocations.html
[15] Ville de Québec City, “Plus de 7 000 jeunes de Québec soutenus par le 2e fonds d’investissement en santé mentale,” November 9, 2023. Retrieved from https://www.ville.quebec.qc.ca/apropos/espace-presse/actualites/fiche_autres_actualites.aspx?id=28583
[16] Mental Health Commission of Canada, Creating Mentally Healthy Cities and Communities, n.d. Retrieved from https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/MHCC_FCM_Brochure_ENG_0.pdf; Mental Health Commission of Canada, Municipalities as Employers, n.d. Retrieved from https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/MHCC_Municipalities_Employers_Facts_Bilingual_2.pdf
[17] Canadian Press, “Tory calls for national summit to tackle mental health crisis,” CBC News, January 25, 2023. Retrieved from https://www.cbc.ca/news/canada/toronto/toronto-mayor-mental-health-1.6725317; City of Toronto, “City of Toronto Mental Health Roundtable calls for increased collaboration and funding to meet city’s urgent challenges,” June 2, 2023. Retrieved from https://www.toronto.ca/news/city-of-toronto-mental-health-roundtable-calls-for-increased-collaboration-and-funding-to-meet-citys-urgent-challenges/
[18] Ontario’s Big City Mayors, “Ontario’s Big City Mayors reiterate call to premier to address the homelessness, mental health and addictions crisis in Ontario,” November 7, 2024. Retrieved from https://www.ontariobigcitymayors.ca/ontarios-big-city-mayors-reiterate-call-to-premier-on-homelessness-mental-health-and-addictions-crisis-in-ontario/
[19] Federation of Canadian Municipalities, “FCM’s Big City Mayors’ Caucus convenes to discuss municipal fiscal framework, homelessness, mental health,” May 25, 2023. Retrieved from https://fcm.ca/en/news-media/news-release/fcms-big-city-mayors-caucus-convenes-discuss-municipal-fiscal-framework-homelessness-mental-health
[20] City of Vancouver, “Decriminalizing simple possession of illicit drugs,” 2025. Retrieved from https://vancouver.ca/people-programs/decriminalizing-simple-possession-of-illicit-drugs-in-vancouver.aspx
[21] Government of Ontario, “Backgrounder: Protecting community safety and connecting more people to addiction recovery care,” News release, August 20, 2024. Retrieved from https://news.ontario.ca/en/backgrounder/1004956/protecting-community-safety-and-connecting-more-people-to-addiction-recovery-care
[22] Government of Ontario, “Backgrounder: The Safer Streets, Stronger Communities Act,” November 18, 2024. Retrieved from https://news.ontario.ca/en/backgrounder/1005354/the-safer-streets-stronger-communities-act
[23] City of Vancouver, “Safe supply statement,” n.d. Retrieved from https://vancouver.ca/people-programs/safe-supply-statement.aspx
[24] Edmonton Suicide Prevention Advisory Committee, Edmonton Suicide Prevention Strategy, 2016. Retrieved from https://www.edmonton.ca/sites/default/files/public-files/assets/PDF/suicide-prevention-strategy.pdf; City of Edmonton, Living Hope: A Community Plan to Prevent Suicide in Edmonton, 2018. Retrieved from https://www.edmonton.ca/sites/default/files/public-files/documents/PDF/living-hope-suicide-prevention-plan.pdf
[25] Saskatchewan Urban Municipalities Association, “New mental health and addictions action plan makes strides, continued collaboration necessary,” media release, November 16, 2023. Retrieved from https://suma.org/pub/media-releases/20231116-cmc_media_advisory_mha.pdf
[26] City of Vancouver, “Memorandum of understanding [permanent modular housing],” July 2020. Retrieved from https://vancouver.ca/files/cov/2020-07-30-permanant-modular-housing-mou.pdf
[27] The Urban Project, “Covid-19, mental health and the role of cities: Virtual roundtables,” April 2021. Retrieved from https://theurbanproject.ca/event/covid-19-mental-health-and-the-role-of-cities/
[28] Ontario Big City Mayors, “Ontario’s Big City Mayors (OBCM), ministers of Finance and Municipal Affairs and Housing meet on key municipal priorities,” February 13, 2023. Retrieved from https://www.ontariobigcitymayors.ca/ontarios-big-city-mayors-obcm-ministers-of-finance-and-municipal-affairs-and-housing-meet-on-key-municipal-priorities/; Ontario Big City Mayors, “Ontario’s Big City Mayors (OBCM) launch election advocacy campaign,” February 13, 2025. Retrieved from https://www.ontariobigcitymayors.ca/ontarios-big-city-mayors-obcm-launch-election-advocacy-campaign/
[29] Government of Canada, “Opioid-and stimulant-related harms in Canada”; Benedikt Fischer, “The continuous opioid death crisis in Canada: Changing characteristics and implications for path options forward,” The Lancet Regional Health: Americas 19,100437 (2023): 1–2. Retrieved from https://doi.org/10.1016/j.lana.2023.100437
[30] Government of Canada, “Opioid- and stimulant-related harms in Canada”; Lisa Belzak and Jessica Halverson, “The opioid crisis in Canada: A national perspective,” Health Promotion and Chronic Disease Prevention in Canada 38,6 (2018): 224–233. Retrieved from https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/health-promotion-chronic-disease-prevention-canada-research-policy-practice/vol-38-no-6-2018/ar-03-eng.pdf
[31] Mark Tyndall, “A safer drug supply: A pragmatic and ethical response to the overdose crisis,” Canadian Medical Association Journal 192,34 (2020): E986–E987. Retrieved from https://www.cmaj.ca/content/192/34/e986; Ryan McNeil, Taylor Fleming, Samara Mayer, Allison Barker, Manal Mansoor, Alex Bestos, Tamar Austin, Sylvia Parusel, Andrew Ivsins, and Jade Boyd, “Implementation of safe supply alternatives during intersecting COVID-19 and overdose health emergencies in British Columbia, Canada, 2021,” American Journal of Public Health 112,S2 (2022): S151–S158. Retrieved from https://doi.org/10.2105/AJPH.2021.306692; Jane Mounteney, Isabelle Giraudon, Gleb Denissov, and Paul Griffiths, “Fentanyls: Are we missing the signs? Highly potent and on the rise in Europe,” International Journal on Drug Policy 26,7 (2015): 626–631. Retrieved from https://doi.org/10.1016/j.drugpo.2015.04.003; Alexis Crabtree, Emily Lostchuck, Mei Chong, Aaron Shapiro, and Amanda Slaunwhite, “Toxicology and prescribed medication histories among people experiencing fatal illicit drug overdose in British Columbia, Canada,” Canadian Medical Association Journal 192,34 (2020): E967–E972. Retrieved from https://doi.org/10.1503/cmaj.200191; Rose A. Rudd, Noah Aleshire, Jon E. Zibbell, and R. Matthew Gladden, “Increases in drug and opioid overdose deaths – United States, 2000–2014,” Morbidity and Mortality Weekly Report (MMWR) 64,50 (2015): 1378–1382. Retrieved from https://doi.org/10.15585/mmwr.mm6450a3
[32] Elaine Hyshka, Jalene Anderson-Baron, Kamagaju Karekezi, Lynne Belle-Isle, Richard Elliott, Bernie Pauly, Carol Strike, Mark Asbridge, Colleen Dell, Keely McBride, Andrew Hathaway, and T. Cameron Wild, “Harm reduction in name, but not substance: A comparative analysis of current Canadian provincial and territorial policy frameworks,” Harm Reduction Journal 14,50 (2017). Retrieved from https://doi.org/10.1186/s12954-017-0177-7; T. Cameron Wild, Bernie Pauly, Lynne Belle-Isle, Walter Cavalieri, Richard Elliott, Carol Strike, Kenneth Tupper, Andrew Hathaway, Colleen Dell, Donald MacPherson, Caitlin Sinclair, Kamagaju Karekezi, Benjamin Tan, and, Elaine Hyshka, “Canadian harm reduction policies: A comparative content analysis of provincial and territorial documents, 2000–2015,” The International Journal on Drug Policy 45 (2017): 9–17. Retrieved from https://pubmed.ncbi.nlm.nih.gov/28454045/
[33] Eric Single, “Defining harm reduction,” Drug and Alcohol Review 14,3 (1995): 287–290. Retrieved from https://doi.org/10.1080/09595239500185371
[34] Single, “Defining harm reduction”; Don C. Des Jarlais, Samuel R. Friedman, and Thomas P. Ward, “Harm reduction: A public health response to the AIDS epidemic among injecting drug users,” Annual Review of Public Health 14 (1993): 413–450. Retrieved from https://pubmed.ncbi.nlm.nih.gov/8323596/; Gordon Roe, “Harm reduction as paradigm: Is better than bad good enough? The origins of harm reduction,” Critical Public Health 15,3 (2005): 243–250. Retrieved from https://doi.org/10.1080/09581590500372188; Harm Reduction International, “What Is Harm Reduction?,” website, accessed July 15, 2024. Retrieved from https://hri.global/what-is-harm-reduction/
[35] Harm Reduction International, “What Is Harm Reduction?”; G. Alan Marlatt, “Harm reduction: Come as you are,” Addictive Behaviors 21,6 (1996): 779–788. Retrieved from https://doi.org/10.1016/0306-4603(96)00042-1; Diane Riley, Ed Sawka, Peter Conley, David Hewitt, Wayne Mitic, Christiane Poulin, Robin Room, Eric Single, and John Topp, “Harm reduction: Concepts and practice. A policy discussion paper,” Substance Use & Misuse 34,1 (1999): 9–24. Retrieved from https://doi.org/10.3109/10826089909035632
[36] Esther J. Aspinall, Dhanya Nambiar, David J. Goldberg, Matthew Hickman, Amanda Weir, Eva Van Velzen, Norah Palmateer, Joseph S. Doyle, Margaret E. Hellard, and Sharon J. Hutchinson, “Are needle and syringe programmes associated with a reduction in HIV transmission among people who inject drugs: A systematic review and meta-analysis,” International Journal of Epidemiology 43,1 (2014): 235–248. Retrieved from https://doi.org/10.1093/ije/dyt243; Ricardo M. Fernandes, Maria Cary, Gonçalo Duarte, Gonçalo Jesus, Joana Alarcão, Carla Torre, Suzete Costa, João Costa, and António Vaz Carneiro, “Effectiveness of needle and syringe programmes in people who inject drugs: An overview of systematic reviews,” BMC Public Health 17,1 (2017): 309. Retrieved from https://doi.org/10.1186/s12889-017-4210-2; Timothy W. Levengood, Grace H. Yoon, Melissa J. Davoust, Shannon N. Ogden, Brandon D. L. Marshall, Sean R. Cahill, and Angela R. Bazzi, “Supervised injection facilities as harm reduction: A systematic review,” American Journal of Preventive Medicine 61,5 (2021): 738–749. Retrieved from https://doi.org/10.1016/j.amepre.2021.04.017; Lisa Chimbar, Yvette Moleta, “Naloxone effectiveness: A systematic review,” Journal of Addictions Nursing 29,3 (2018): 167–171. Retrieved from https://doi.org/10.1097/JAN.0000000000000230; Amir Razaghizad, Sarah B. Windle, Kristian B. Filion, Genevieve Gore, Irina Kudrina, Elena Paraskevopoulos, Jonathan Kimmelman, Marc O. Martel, and Mark J. Eisenberg, “The effect of overdose education and naloxone distribution: An umbrella review of systematic reviews,” American Journal of Public Health 111,8 (2021): e1–e12. Retrieved from https://doi.org/10.2105/AJPH.2021.306306
[37] Health Canada, “Canadian drugs and substances strategy: Overview,” last modified July 27, 2024. Retrieved from https://www.canada.ca/en/health-canada/services/substance-use/canadian-drugs-substances-strategy.html
[38] Hyshka et al., “Harm reduction in name”; Wild et al., “Canadian harm reduction policies”; Carol Strike, Tara Marie Watson, Gillian Kolla, Rebecca Penn, and Ahmed M. Bayoumi, “Ambivalence about supervised injection facilities among community stakeholders,” Harm Reduction Journal 12,26 (2015). Retrieved from https://doi.org/10.1186/s12954-015-0060-3; Tony Davis, “Charlottetown council votes against supervised injection site,” CBC News, September 26, 2023. Retrieved from https://www.cbc.ca/news/canada/prince-edward-island/pei-charlottetown-homeless-emergency-housing-extended-outreach-centre-1.6977926
[39] City of Toronto, “Naloxone Administration,” 2020. Retrieved from https://www.toronto.ca/city-government/accountability-operations-customer-service/city-administration/corporate-policies/people-equity-policies/naloxone-administration/
[40] Jonathan Ore, “Why staff at an Ontario cottage country restaurant took naloxone training,” CBC Radio, April 2024. Retrieved from https://www.cbc.ca/radio/whitecoat/muskoka-opioid-workplace-naloxone-training-1.7168235
[41] Madeleine Cummings, “City of Edmonton policy forbids most employees from administering naloxone during work hours,” CBC News, December 22, 2022. Retrieved from https://cbc.ca/news/canada/edmonton/city-of-edmonton-naloxone-policy-1.6693081
[42] Canadian Centre for Occupational Health and Safety, First Aid – Administering Naloxone (Naloxone Hydrochloride), 2020. Retrieved from https://www.ccohs.ca/oshanswers/hsprograms/firstaid/firstaid_naloxone.html; Christa R. Lewis, Hoa T. Vo, and Marc Fishman, “Intranasal naloxone and related strategies for opioid overdose intervention by nonmedical personnel: A review,” Substance Abuse and Rehabilitation 8 (2017): 79–95. Retrieved from https://doi.org/10.2147/SAR.S101700
[43] Canadian Centre for Occupational Health and Safety, First Aid – Administering Naloxone.
[44] Mariana Valverde, “Taking ‘land use’ seriously: Toward an ontology of municipal law,” Law Text Culture, 9 (2005). Retrieved fromhttps://doi.org/10.14453/ltc.543
[45] City of Edmonton, First Time Electronic Dance Music Event Checklist, n.d. Retrieved from https://www.edmonton.ca/sites/default/files/public-files/documents/PDF/FirstTimeElectronicDanceMusicEventChecklist.pdf?cb=1720716855
[46] Mariana Valverde, “Taking ‘land use’ seriously.”
[47] City of Edmonton, Bylaw 20700, Public Spaces Bylaw. Retrieved from https://www.edmonton.ca/sites/default/files/public-files/BL20700.pdf?cb=1740561351
[48] Lauren Boothby, “Drink up: Edmonton allows alcohol at some park sites permanently,” Edmonton Journal, February 27, 2023. Retrieved from https://edmontonjournal.com/news/local-news/drink-up-edmonton-allows-alcohol-in-some-park-sites-permanently
[49] Scott E. Bernstein and Darcie Bennett, “Zoned out: ‘NIMBYism,’ addiction services, and municipal governance in British Columbia,” International Journal of Drug Policy 24,6 (2013): e61–e65. Retrieved from https://doi.org/10.1016/j.drugpo.2013.04.001
[50] Valverde, “Taking ‘land use’ seriously.”
[51] Association of Municipalities Ontario, A Compendium of Municipal Health Activities and Recommendations, 2019. Retrieved from https://www.amo.on.ca/sites/default/files/assets/DOCUMENTS/Reports/2019/CompendiumofMunicipalHealthActivitiesandRecommendations20190118.pdf
[52] City of Regina, “Harm reduction grant,” n.d. Retrieved from https://www.regina.ca/about-regina/grants-scholarships/community-investment-grants/social-development-grants/#outline-harm-reduction-grant
[53] Association of Local Public Health Agencies, “Public health units,” n.d. Retrieved from https://www.alphaweb.org/page/PHU; See also Eidelman, Gabriel, Kass Forman, Tomas Hachard, and Enid Slack, eds. 2022. The Municipal Role in Public Health. Who Does What Series, No. 4 (Toronto: Institute on Municipal Finance and Governance).
[54] Peterborough Drug Strategy, Consumption and Treatment Services: Community Engagement Survey Report, 2019. Retrieved from https://www.fourcast.ca/wp-content/uploads/2022/06/CTS-Community-Engagement-Survey-Report-2019.pdf; Fourcast, Community Impact Report, 2022. Retrieved from http://www.fourcast.ca/wp-content/uploads/2022/09/Community_Impact_Report_CTS_Sept_2022.pdf; Cayley Russell, Sameer Imtiaz, Farihah Ali, Tara Elton-Marshall, and Jürgen Rehm, “‘Small communities, large oversight’: The impact of recent legislative changes concerning supervised consumption services on small communities in Ontario, Canada,” International Journal of Drug Policy, 82,102822 (2020). Retrieved from https://doi.org/10.1016/j.drugpo.2020.102822
[55] Fourcast, CTS@220: A Year in Review (2022–2023), 2023. Retrieved from https://cfgp.ca/wp-content/uploads/2023/07/CTSat220-Year-in-Review-June-2023.pdf
[56] Tobias Kammersgaard, “Harm reduction policing: From drug law enforcement to protection,” Contemporary Drug Problems 46,4 (2019): 345–362. Retrieved from https://doi.org/10.1177/0091450919871313
[57] Will Small, Thomas Kerr, John Charette, Martin T. Schechter, and Patricia M. Spittal, “Impacts of intensified police activity on injection drug users: Evidence from an ethnographic investigation,” The International Journal of Drug Policy 17 (2006): 85–95. Retrieved from https://doi.org/10.1016/j.drugpo.2005.12.005; Evan Wood and Thomas Kerr, “Measuring the public health impact of police activities on illicit drug users,” International Journal of Drug Policy 16 (2005): 148–149. Retrieved from https://doi.org/10.1016/j.drugpo.2005.04.001; Joanne Csete, Adeeba Kamarulzaman, Michel Kazatchkine, Frederick Altice, Marek Balicki, Julia Buxton, Javier Cepeda, Megan Comfort, Eric Goosby, João Goulão, Carl Hart, Thomas Kerr, Alejandro Madrazo Lajous, Stephen Lewis, Natasha Martin, Daniel Mejía, Adriana Camacho, David Mathieson, Isidore Obot, Adeolu Ogunrombi, Susan Sherman, Jack Stone, Nandini Vallath, Peter Vickerman, Tomáš Zábranský, and Chris Beyrer, “Public health and international drug policy,” The Lancet 387,10026 (2016): P1427–1480. Retrieved from https://doi.org/10.1016/S0140-6736(16)00619-X
[58] Small et al., “Impacts of intensified police activity”; Jonathan P. Caulkins and Peter Reuter, “Towards a harm-reduction approach to enforcement,” Safer Communities 8 (2009): 9–23. Retrieved from https://doi.org/10.1108/17578043200900003
[59] Vanessa Gruben, Elaine Hyshka, Matthew Bonn, Chelsea Cox, Marilou Gagnon, Adrian Guta, Martha Jackman, Jason Mercredi, Akia Munga, Eugene Oscapella, Carol Strike, and Hakique Virani, “Urgent and long overdue: legal reform and drug decriminalization in Canada,” FACETS 9 (2024): 1–28. Retrieved from https://doi.org/10.1139/facets-2022-0080; Rebecca Jesseman and Doris Payer, Decriminalization: Options and Evidence (Ottawa: Canadian Centre on Substance Use and Addiction, 2018). Retrieved from https://www.ccsa.ca/sites/default/files/2019-04/CCSA-Decriminalization-Controlled-Substances-Policy-Brief-2018-en.pdf
[60] Csete et al., “Public health and international drug policy;” Caulkins and Reuter, “Towards a harm-reduction approach to enforcement;” The Lancet Editorial, “Drug decriminalisation: Grounding policy in evidence,” The Lancet 402,10416 (2023): 1941. Retrieved from https://doi.org/10.1016/S0140-6736(23)02617-X
[61] Special Purpose Committee on the Decriminalization of Illicit Drugs, Decriminalization for Simple Possession of Illicit Drugs: Exploring Impacts on Public Safety and Policing (Kanata: Canadian Association of Chiefs of Police, 2020). Retrieved from https://www.cacp.ca/_Library/resources/202007081322111653496031_decriminalizationreportjuly2020.pdf
[62] Sean Amato, “Edmonton moves forward on decriminalizing ‘simple personal possession’ of drugs,” CTV News: Edmonton,April 11, 2022. Retrieved from https://edmonton.ctvnews.ca/edmonton-moves-forward-on-decriminalizing-simple-personal-possession-of-drugs-1.5857543#:~:text=Edmonton%20moves%20forward%20on%20decriminalizing%20’simple%20personal%20possession’%20of%20drugs&text=Edmonton%20city%20councillors%20took%20a,drug%20poisoning%20injuries%20and%20deaths.%22; Paula Tran, “Drug decriminalization in province ‘premature’ says Alberta police chiefs,” Global News,February 22, 2023. Retrieved from https://globalnews.ca/news/9504274/drug-decriminalization-premature-alberta-police-chiefs/
[63] Farihah Ali, Justine Law, Cayley Russell, Jean-Francois Crépault, João Castel-Branco Goulão, Kurt Lock, and Jürgen Rehm, “Navigating the nexus between British Columbia’s public consumption and decriminalization policies of illegal drugs,” Health Research Policy and Systems 22,60 (2024). Retrieved from https://doi.org/10.1186/s12961-024-01150-6
[64] Etienne Blais, Jacinthe Brisson, François Gagnon, and Sophie-Anne Lemay, “Diverting people who use drugs from the criminal justice system: A systematic review of police-based diversion measures,” International Journal of Drug Policy 105,103697 (2022). Retrieved from https://doi.org/10.1016/j.drugpo.2022.103697
[65] Canadian Drug Policy Coalition, Canadian HIV/AIDS Legal Network, International Centre for Science in Drug Policy, and Canadian Association of People Who Use Drugs, ACTION = LIFE: Call for an Immediate Response to National Crisis of Opioid Overdose Deaths, 2016. Retrieved from http://www2.cdnaids.ca/wp-content/uploads/CDPC-LN_Overdose-Crisis-2_CalltoAction_August31-EN.pdf
[66] Bernstein and Bennett, “Zoned out.”
[67] Wood and Kerr, “Measuring the public health impact.”
[68] Centers for Disease Control and Prevention (CDC), Mental Health (Atlanta: CDC, n.d.).Retrieved from https://www.cdc.gov/mental-health/?CDC_AAref_Val=https://www.cdc.gov/mentalhealth/index.htm
[69] World Health Organization (WHO). Health and Well-Being (Geneva: WHO, n.d.). Retrieved from https://www.who.int/data/gho/data/major-themes/health-and-well-being#:~:text=Mental%20health%20is%20a%20state,to%20his%20or%20her%20community
[70] C. L. Keyes, “The next steps in the promotion and protection of positive mental health,” Canadian Journal of Nursing Research 42,3 (2010): 17–28. Retrieved from https://psycnet.apa.org/record/2010-21950-003
[71] A. M. Doherty and F. Gaughran, “The interface of physical and mental health,” Social Psychiatry and Psychiatric Epidemiology 49 (2014): 673–682. Retrieved from https://doi.org/10.1007/s00127-014-0847-7
[72] E. Chesney, G. M. Goodwin, and S. Fazel, “Risks of all‐cause and suicide mortality in mental disorders: A meta‐review,” World Psychiatry 13,2 (2014): 153–160. Retrieved from https://doi.org/10.1002/wps.20128
[73] K. McKenzie and T. Harpham (eds.), Social Capital and Mental Health (London: Jessica Kingsley Publishers, 2006). Retrieved from https://psycnet.apa.org/record/2006-21129-000
[74] K. L. Lim, P. Jacobs, A. Ohinmaa, D. Schopflocher, and C. S. Dewa, “A new population-based measure of the economic burden of mental illness in Canada,” Chronic Diseases in Canada 28,3 (2008): 92–98. Retrieved from https://pubmed.ncbi.nlm.nih.gov/18341763/
[75] R. Mezzina, V. Gopikumar, J. Jenkins, B. Saraceno, and S. P. Sashidharan, “Social vulnerability and mental health inequalities in the ‘Syndemic’: Call for action,” Frontiers in Psychiatry 13 (2022): 894370. Retrieved from https://doi.org/10.3389/fpsyt.2022.894370
[76] K. W. Liming, “Examining the differing effects of economic hardship and poor maternal wellbeing on cumulative exposure to adverse childhood experiences,” Journal of Child & Adolescent Trauma 12,3 (2019): 307–321. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7163802/
[77] J. B. Kirkbride, D. M. Anglin, I. Colman, J. Dykxhoorn, P. B. Jones, P. Patalay, A. Pitman, E. Soneson, T. Steare, T. Wright, and S. L. Griffiths, “The social determinants of mental health and disorder: Evidence, prevention and recommendations,” World Psychiatry 23,1 (2024 Feb): 58–90. Retrieved from https://pubmed.ncbi.nlm.nih.gov/38214615/; J. Zhu, N. Racine, C. Devereux, D. C. Hodgins, and S. Madigan, “Associations between adverse childhood experiences and substance use: A meta-analysis,” Child Abuse & Neglect (2023): 106431. Retrieved from https://doi.org/10.1016/j.chiabu.2023.106431
[78] K. A. McLaughlin, J. G. Green, M. J. Gruber, N. A. Sampson, A. M. Zaslavsky, and R. C. Kessler, “Childhood adversities and first onset of psychiatric disorders in a national sample of US adolescents,” Archives of General Psychiatry 69,11 (2012): 1151–1160. Retrieved from 10.1001/archgenpsychiatry.2011.2277; R. C. Kessler, K. A. McLaughlin, J. G. Green, M. J. Gruber, N. A. Sampson, A. M. Zaslavsky, … and D. R. Williams, “Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys,” The British Journal of Psychiatry 197(5) (2010): 378–385. Retrieved from https://doi.org/10.1192/bjp.bp.110.080499
[79] G. Rose, “Sick individuals and sick populations,” International Journal of Epidemiology 30,3 (2001): 427–432. Retrieved from https://doi.org/10.1093/ije/30.3.427
[80] Federation of Canadian Municipalities and Wellesley Institute, FCM Roadmap.
[81] E. G. Castillo, R. Ijadi-Maghsoodi, S. Shadravan, E. Moore, M. O. Mensah III, M. Docherty, … and K. B. Wells, “Community interventions to promote mental health and social equity,” Focus 18(1) (2020): 60–70. Retrieved from https://doi.org/10.1176/appi.focus.18102
[82] Kirkbride et al., “The social determinants of mental health and disorder.”
[83] Centre for Addiction and Mental Health (CAMH), “Mental illness and addiction: Facts and statistics” (Toronto: Centre for Addiction and Mental Health, n.d.). Retrieved from https://www.camh.ca/en/driving-change/the-crisis-is-real/mental-health-statistics
[84] S. Elliott and R. Cheff. Thriving in the City for Families: A Framework for Income and Health (Toronto: Wellesley Institute, 2021). https://www.wellesleyinstitute.com/wp-content/uploads/2021/08/Thriving-Familes-Framework-Report.pdf
[85] L. Lowe, D. Fearon, A. Adenwala, and D. Wise Harris. The State of Mental Health in Canada 2024: Mapping the Landscape of Mental Health, Addictions and Substance Use Health (Toronto: Canadian Mental Health Association, 2024). Retrieved from https://cmha.ca/wp-content/uploads/2024/11/CMHA-State-of-Mental-Health-2024-report.pdf
[86] City of Toronto. Our Health, Our City.
[87] F. Scott, M. Tolentino, et al., Thrive Toronto: A Mental Health Plan for Our City (Toronto: Wellesley Institute, 2023). Retrieved from https://thriveto.ca/wp-content/uploads/2023/10/Thrive_Toronto_Mental_Health_Plan_OCT_2023.pdf
[88] F. Scott et al., Thrive Toronto.
[89] City of Calgary, A Community of Connections: Calgary Mental Health and Addiction Community Strategy and Action Plan 2021–2023, 2021. Retrieved from https://pub-calgary.escribemeetings.com/filestream.ashx?DocumentId=158810
[90] City of New York, Thrive NYC: A Roadmap for Mental Health for All,2019. Retrieved from https://mentalhealth.cityofnewyork.us/wp-content/uploads/2019/08/Thrive-Roadmap.pdf
[91] Thrive LDN, Thrive LDN’s Impact Report for 2022–23, 2023. Retrieved from https://thriveldn.co.uk/communications/toolkits-and-resources/toolkit/thrive-ldn-impact-report-2022-23/
[92] Thrive Toronto and Wellesley Institute, Appendix D: Safe TO: Roadmap to become a Trauma-Informed City (Toronto: City of Toronto, 2021). Retrieved from https://www.toronto.ca/legdocs/mmis/2021/ex/bgrd/backgroundfile-168554.pdf
[93] Federation of Canadian Municipalities and Wellesley Institute, FCM Roadmap.
[PR1]Pull quote:
Although not formally responsible for mental health, municipal governments in Canada are nevertheless at the front lines of what many experts describe as a mental health crisis.
[PR2]Pull quote:
As a result of both financial and legal constraints, municipal governments must work closely with provincial health authorities.
[PR3]Pull quote:
Despite being the nearest order of government to the daily lives of local citizens, municipalities often do not have any formal harm reduction policies.
[PR4]Where possible, municipalities should consider applying a harm reduction lens to relevant policies and procedures to ensure that they promote the health and well-being of people who use substances.
[PR5]Pull quote:
As key catalyzers of concerted policy adoption, municipalities are well positioned to lead the change through inclusive and non-stigmatizing approaches to substance use, including the consistent application of regulations applied to other health and social services.
[PR6]Pull quote:
The relationship between mental health and social capital is cyclical: poor mental health erodes social capital, and the deterioration of social capital, in turn, detrimentally impacts the overall well-being of communities.
OR THE LINE BELOW???
[DG7]Yes
[PR8]Pull quote:
While mental health funding varies across provinces and municipalities, federal spending in Canada lags behind that of other OECD countries.
[PR9]Pull quote:
Although there is much more all municipalities can do to improve their residents’ well-being, they should not have to do this work alone, given that many policy and funding levers are under the jurisdiction of provincial governments in Canada.
Footnote
Click to scroll to footnotes